Currently, I'm on break between 1st and 2nd year. It's hard to believe, but I graduate nursing school next May! Just 9 months away! I can barely believe nursing school is almost halfway done.
It had been so long since I'd had a break with nothing to do, that my first week of break I had no idea what to do. I'm used to always having to be studying so suddenly not having to study and getting to decide what *I* want to do was extremely hard. I had no idea what to do.
Anyway, I decided to write a post to encourage students starting nursing school this fall. If you're like I was, you're excited and nervous and have no idea what to expect. If your program is anything like mine, then hopefully my recommendations and tips will be helpful!
Warning: your first day of school will be overwhelming! There is so much the teachers will cover that first day. I know I was stressed out within 20 minutes of class starting because we started with the syllabus. If your teachers are anything like mine, they will like to scare you. My teachers started with the "don'ts" and the "this will get you kicked out of nursing school." By the end of the day, I was convinced I'd be kicked out by the end of the week.
Don't worry! You can do this!
When you get your syllabus, take the time to go through and read everything, write every single due date down on every single calendar you own, highlight the important stuff (yes, everything's "important," but highlight the "drop dead" dates), and post it in places you'll see it. My teachers made us calendars with the class schedules so I taped the calendars to my desk so I'd see it every day. I also wrote every possible due date onto that calendar. It was my most important calendar. And to keep me motivated, I crossed off every day that passed with a pretty highlighter. (If you haven't noticed, I'm right brained and I LOVE color! The more colors I see, the more I get excited. Needless to say, I highlight everything - my notes, my calendars, my textbooks, etc.)
For clinicals, make sure to print off everything you need for clinicals at least the night before. Don't wait until the morning of clinicals to try and print everything because Murphy's Law will take effect and your printer will die. Also, lay out everything you need the night before. I always put my uniform together on one hanger and stick all my pens and penlights and stethoscope and paperwork in my pockets and stick the hanger in the bathroom so all I have to do at 4:30am is roll out of bed and get straight into the shower. Then, everything I need is right there.
Make friends with your classmates! They are your biggest support group. You will spend more time with your classmates than with your family. There will be classmates you love, classmates you like, classmates, you don't like or dislike, and classmates you don't particularly like. But please make friends with your seat mates! The girl I sit next to has quickly become one of my best friends. We'll spend the night at each others' houses, study together, go out to lunch, practice skills together, text each other about everything, cry together, laugh together, roll our eyes at each other, etc. A buddy in class is invaluable!
Also, it's ok to take an afternoon off and not think about nursing school occasionally. Not frequently, but only occasionally. I'd do it about once a month, whenever I'd hit a wall and think "that's it! I'm going to quit!" It's ok to just take an afternoon off, go to a movie, go shopping, whatever you need to do to relax!
One thing I have found extremely helpful is to do practice NCLEX questions. I've found free online NCLEX questions and there's also apps with practice NCLEX questions. The more questions you do, the better you'll do.
Lastly, don't forget to relax and have fun! Nursing school is extremely stressful and hard but it is worth it! You will get to see and do so much and you will feel so overwhelmed and tired and confused. There is nothing like it. I love it but I can't wait to graduate in May!
Hopefully next week I'll get to post "Advice for New Nursing Students, part 2" and talk about clinicals.
 |
| You will feel like this after every single test |
 |
| Nursing humor is its own breed |
 |
| This is hilarious! |
 |
| The only stories that gross me out are ones with oozing dead fluids...or maggots in your skin... |
 |
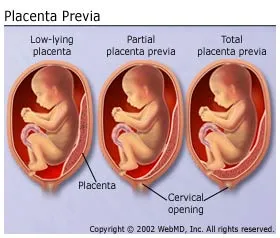
| This is what your textbooks will look like |
 |
| You will eventually cry at clinicals or work |
 |
| You will save a life |
 |
| And this will be your life! (And I have gotten fat in nursing school) |